

INTRODUCTION:
Autoantibody effects of monoclonal proteins have been described in multiple organ systems. We previously found a 5-fold higher prevalence than expected of monoclonal gammopathy (MG) in adults with TMA (21% versus 4.2%; Ravindran A et al, Kidney Int 2017). Here we investigated the prevalence of MG in patients undergoing evaluation for TMA with an ADAMTS13 (a disintegrin and metalloprotease with a thrombospondin type 1 motif, member 13) activity assay performed as part of routine clinical care to evaluate for a signal of possible autoantibody pathophysiology in patients with immune thrombotic thrombocytopenic purpura (iTTP).
METHODS:
WAfter IRB approval, waste plasma samples from patients who had ADAMTS13 activity and inhibitor assay (Lifecodes, ATS-13, Immucor) were archived. Eligible patients included those with the following: i) ADAMTS13 activity level < 30% (n=26), ii) ADAMTS13 activity level >30% but with prior documentation of a value < 30% (n=4). A control cohort (n=49) of patients with ADAMTS13 activity level >30% (and no prior samples with a level < 30% recorded) was also included. Matrix-assisted laser desorption/ionization-time of flight mass spectrometry detection (MALDI-TOF) was used for MG assessment. Mass spectrometry findings of only an IgG kappa MG appearing consistent with rituximab were reviewed and considered negative for MG if the patients had received rituximab prior to sample collection. Medical records were retrospectively reviewed and the following patients were excluded: i) <18 years of age (n=4), ii) iTTP in remission (n=4) at the time of sample collection, and iii) absence of microangiopathy (n=11).
RESULTS:
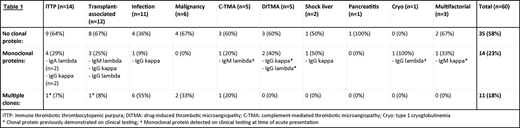
Sixty patients met eligibility criteria with the following final diagnoses: iTTP (n=14), transplant-associated TMA (n=12), infection (n=11), malignancy (n=6), complement-mediated TMA (n=5), drug-induced TMA (DITMA; n=5), shock liver (n=2), pancreatitis (n=1), cryoglobulinemia (n=1), and multifactorial (n=3). The median age was 56.5 years (yr) (standard deviation 14.4, range18-81) and 58% of patients were female. The median age was similar among patients with (57 yr) and those without MG (56 yr). Median ADAMTS-13 activity of the whole study population was 52% (0-100%); 6/14 patients with an inhibitor screen performed on the same sample had a positive result; median titer was 1.2 Bethesda units (range <0.4 - 2.8).
Treatments of the acute presentation included corticosteroids (n=32), plasma exchange (n=21), rituximab (n=9), and eculizumab (n=4). None of these patients received a multiple myeloma-type treatment regimen as part of their acute management.
A MG was identified in 25 patients: monoclonal in 14 patients, biclonal in 10 patients, and triclonal in 1 pt. Among the 14 patients with a single monoclonal protein, the distribution of heavy and light chains was as follows: IgG (9; 64%), IgM (3; 21%), IgA (2; 14%), lambda (8; 57%), kappa (6; 43%). Receipt of immune-modifying treatment at the time of sample draw was identified in 24 patients (9/25 with a monoclonal protein, 15/35 without a monoclonal protein; not statistically significant by 2-tail Fisher's exact test [p=0.79]), including cancer-directed therapy (n=9), graft-versus-host disease prophylaxis (n=8), solid organ transplant anti-rejection therapy (n=5), and autoimmune disease treatment (n=2). Overall, the proportion of patients with monoclonal gammopathy was similar between iTTP and other diagnoses, detailed in Table 1.
Among the 14 pt with iTTP, 4 had a monoclonal protein (IgG kappa [n=2], IgA lambda [n=2]). Additionally, 1 pt with iTTP had biclonal proteins (IgG kappa and IgA kappa), which was consistent with a known prior history of monoclonal gammopathy of undetermined significance. A monoclonal protein was present in 2 of the 6 pt with a detectable inhibitor titer (0.6 and <0.4 Bethesda units).
CONCLUSIONS:
Patients undergoing evaluation for iTTP with ADAMTS-13 activity testing had a high prevalence of monoclonal proteins across variable underlying diagnoses. In this heterogeneous cohort there was no significant association between iTTP and the presence of MG to support an autoantibody pathophysiologic role.
Murray:The Binding Site: Patents & Royalties: Patent Use of Mass Spec to identify monoclonal proteins licensed to The Binding Site. Pruthi:HEMA Biologics: Honoraria; Instrumentation Laboratory: Honoraria; Merck: Honoraria; CSL Behring: Honoraria; Genentech Inc.: Honoraria; Bayer Healthcare: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal